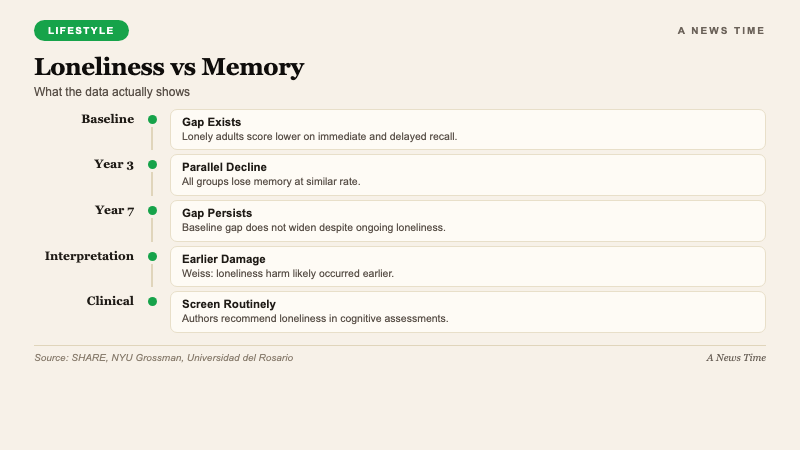
Loneliness may quietly damage memory in older adults, but it does not necessarily speed up cognitive decline, according to research published this month in Aging & Mental Health and covered by the New York Post on . Researchers from Colombia, Spain, and Sweden analyzed data from more than 10,000 adults aged 65 to 94 across 12 European countries and found that those who reported higher loneliness performed worse on memory tests at the start of the study. Over seven years of follow-up, however, the rate of memory decline was similar across all loneliness groups. The finding separates two questions that public health discourse often conflates: whether loneliness causes dementia, and whether loneliness is associated with worse cognitive performance.
For aging adults, clinicians, and family members navigating cognitive health, the study's implication is specific. Loneliness appears to influence where memory performance is, not how quickly it changes going forward. That distinction matters for intervention strategy. It also reframes loneliness as a potential early-life risk factor with cumulative effects, rather than an acute accelerator of late-life decline.
What the Study Actually Measured
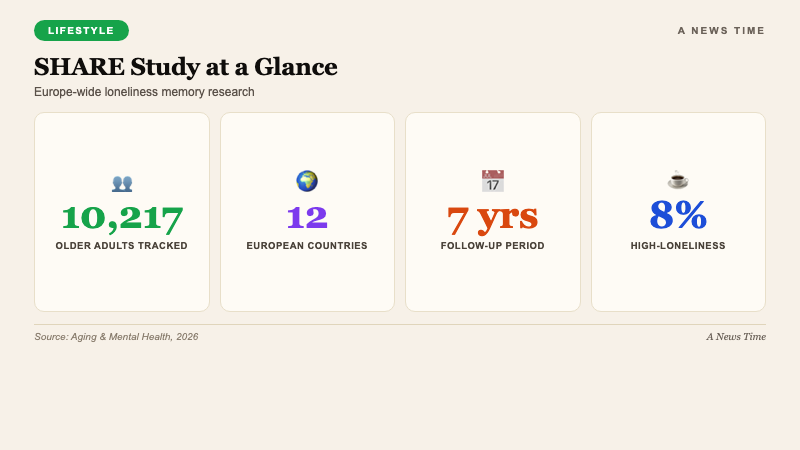
The research used the Survey of Health, Ageing and Retirement in Europe (SHARE), a long-running longitudinal study that has tracked adults across multiple European countries since 2004. The specific cohort for this analysis included 10,217 adults aged 65 to 94 who participated between 2012 and 2019. Loneliness was assessed using three standard questions about how often participants felt isolated, left out, or lacking companionship. Memory performance was measured by asking participants to recall words immediately after exposure and again after a delay.
| Element | Value |
|---|---|
| Sample size | 10,217 adults |
| Age range | 65-94 |
| Countries | 12 European countries |
| Follow-up period | 7 years (2012-2019) |
| Data source | SHARE |
| Publication | Aging & Mental Health, 2026 |
| High-loneliness prevalence | ~8% of sample |
About 8% of participants reported high loneliness at the study's start. That high-loneliness group tended to be older on average, more likely to be female, and more likely to have conditions including depression, high blood pressure, and diabetes. All three of those conditions independently associate with memory performance, which creates an interpretive complication the study authors and outside commentators both acknowledge.
The Surprising Non-Finding
Lead author Luis Carlos Venegas-Sanabria of the Universidad del Rosario's School of Medicine and Health Sciences flagged what the researchers did not find as the more interesting result. Memory decline over the seven-year follow-up occurred at a similar rate regardless of how lonely participants felt at baseline. The baseline gap between high-loneliness and low-loneliness groups persisted. Both groups declined from their respective starting points at roughly the same slope.
"The finding that loneliness significantly impacted memory, but not the speed of decline in memory over time was a surprising outcome. It suggests that loneliness may play a more prominent role in the initial state of memory than in its progressive decline."
Dr. Luis Carlos Venegas-Sanabria, Universidad del Rosario School of Medicine and Health Sciences
This pattern separates two common interpretations of loneliness research. The first, that loneliness causes ongoing cognitive damage that compounds over time, would predict a steeper slope of decline in lonely participants. The second, that loneliness correlates with earlier cognitive damage but does not continue to accelerate decline, is what the data supports. The study does not definitively prove either interpretation, but it shifts the weight of evidence toward the second.
Why the Earlier-in-Life Framing Matters
Jordan Weiss, a scientific advisor at Assisted Living Magazine and a professor at NYU Grossman School of Medicine who was not involved in the research, offered the interpretation that explains the baseline gap. "It likely means loneliness does its damage earlier in life, well before people show up in a study like this at 65-plus," Weiss told Fox News Digital. "By the time you're measuring someone in their late 60s, decades of social connection patterns are already baked in."
Weiss's framing points to a practical implication that differs from the public-health messaging most commonly associated with loneliness research. If loneliness does its damage early, interventions aimed at reducing loneliness in elderly populations may show smaller effects on cognitive outcomes than expected. Interventions that address social isolation in middle-aged and even younger adults, on the other hand, might be more consequential for long-term cognitive health, even though that timeline is harder to study and slower to measure.
What the Findings Do Not Mean
Clinicians and researchers warned that the non-finding on decline rate should not be read as evidence that loneliness is harmless. The baseline association between high loneliness and worse memory is itself a meaningful public-health finding. The co-occurring conditions (depression, high blood pressure, diabetes) also matter because they are modifiable, which creates intervention pathways that indirectly address loneliness-linked cognitive risk.
Amy Morin, a Florida-based psychotherapist, characterized the evidence base as showing "a link between loneliness and cognitive decline but no direct evidence of a cause and effect relationship." She added that loneliness may be "a symptom of other underlying mental or physical health issues" rather than the root problem. That framing suggests interventions should target the broader constellation of health issues rather than loneliness alone.
"It's important to be proactive about social activities. Joining a book club, having coffee with a friend, or attending faith-based services can be a powerful way to maintain connections in older age."
Amy Morin, psychotherapist and author
The Clinical Recommendation
The study authors recommended that loneliness screening be incorporated into routine cognitive assessments. That is a lower-cost, lower-intensity intervention than most of the options currently used in primary care. A brief three-question loneliness screen during an annual wellness visit adds minimal time and could identify patients who would benefit from social-prescribing referrals, community-center connections, or mental-health consultation.
Social prescribing, which has expanded in the UK's National Health Service and in pilot programs in the US and Canada over the past decade, is the specific clinical pathway most directly relevant to this research. A primary-care provider identifying a lonely older patient can refer to a community-based social-prescribing coordinator who helps connect the patient with group activities, volunteer opportunities, or peer networks. The evidence base for social prescribing is still developing, but the intervention is low-risk and aligned with the study's findings on baseline cognitive correlations.
What Loneliness Actually Looks Like at 65+
The study's 8% high-loneliness prevalence is consistent with other surveys of older adults in developed economies. Prevalence tends to rise in the 75-and-older subgroup, where cohort effects of widowhood, physical limitations on mobility, and shrinking social networks become more pronounced. The women-skewed composition of the high-loneliness group reflects the demographic reality that women outlive men by several years on average, which increases exposure to widow-related isolation.
Geographic variation matters too. Within the 12-country European sample, loneliness prevalence varies measurably between Northern and Southern European countries. Mediterranean cultures with stronger multi-generational household structures tend to show lower loneliness prevalence among older adults than Nordic countries with higher rates of independent living. The US data, though not part of this study, tracks closer to Nordic patterns than to Mediterranean ones.
Frequently Asked Questions
Does loneliness cause dementia?
The evidence shows a link between loneliness and worse cognitive performance but does not establish direct causation. The new study specifically finds that loneliness correlates with worse baseline memory but not with faster rate of memory decline in older adults over a seven-year period.
How was the study designed?
Researchers analyzed 10,217 adults aged 65 to 94 across 12 European countries between 2012 and 2019 using the Survey of Health, Ageing and Retirement in Europe. Memory was assessed through immediate and delayed word-recall tests. Loneliness was assessed through a three-item self-report.
What did the study find about loneliness severity?
About 8% of participants reported high loneliness at baseline. That group tended to be older, more likely to be female, and more likely to have depression, high blood pressure, or diabetes than less-lonely participants.
What can older adults do about loneliness?
Experts recommend proactive social engagement including club memberships, regular social meetings with friends, and faith-based or community-center participation. Primary-care providers can screen for loneliness and refer to social-prescribing programs where available.
When should loneliness interventions begin?
The study suggests loneliness may do its cognitive-related damage earlier in life, which implies interventions aimed at reducing loneliness in middle age or earlier could have larger long-term effects than interventions that wait until the 65-plus age range.
What to Watch
Future research will test whether loneliness interventions in middle-aged adults show measurable effects on cognitive outcomes decades later. The ongoing SHARE cohort provides a framework for extended follow-up as current participants age further. US-based longitudinal studies including the Health and Retirement Study will likely publish parallel analyses using their own cohorts. Clinical integration of loneliness screening into routine primary care is the most actionable near-term implication of this line of research.